Introduction to Bipolar Disorder
Types of bipolar disorder
The DSM-5 has four classifications for bipolar disorder.

Characterized by both manic and depressive episodes.21,22
Characterized by both hypomanic and depressive episodes.21,22
Related to bipolar disorder, it features both hypomanic and depressive symptoms that never meet the full criteria for diagnosis of hypomanic or depressive episodes.21 Individuals can also experience impulsive and anxious behaviors.26

Bipolar disorder may result from medications, substance use, or another medical disorder. Some individuals may show bipolar-like symptoms that do not fit the criteria for bipolar I, bipolar II, or cyclothymic disorder. These individuals may be given a diagnosis of other specified bipolar and related disorder.21
Introduction to Bipolar Disorder
What is the burden of bipolar disorder?
Prevalence
In the U.S., 1.1% of adults aged 18–64 will be diagnosed with bipolar I disorder and 1.4% will be diagnosed with bipolar II disorder at some point in their lifetime27, with males and females being equally affected. It was estimated that in 2015 there were 2,477,737 adults in the U.S. with bipolar I disorder.28 According to data from Substance Abuse and Mental Health Services Administration, in 2017, 567,216 adults in the U.S. received a bipolar disorder diagnosis.29
Functional Impairment
Your patients with bipolar disorder may experience a decrease in quality of life and have difficulty performing regular tasks, having healthy relationships, and retaining employment,21,30 even during periods of euthymia.21,31 Beyond its effects on mood, people with bipolar disorder can experience cognitive impairment, and people with psychosis can experience a greater decline in cognitive function.31
Impairments in processing speed, working memory, and attention can lead to difficulties in thinking, focusing, and responding to what is happening around them.31 Your patients may also experience verbal and episodic memory deficiencies and not be able to easily remember words or details of specific events.31 Executive function, such as seeing tasks through from start to finish, may also be negatively impacted.31 People with bipolar disorder may also find it difficult to correctly read the emotions of other people.32
These effects of bipolar disorder can negatively impact relationships32 and may lead to unemployment.33 In 2002, individuals with bipolar disorder lost an average of 27.7 days of work due to absenteeism, and lost the equivalent of 35.3 workdays due to presenteeism (using DSM-IV criteria).34 In 2017, 17.9% of adults with bipolar disorder reported being unemployed.29 People with bipolar disorder may also experience stigma and exclusion in the workplace due to misconceptions about their condition, and this discrimination is associated with higher rates of unemployment.33
Bipolar disorder may impact more than your patient. Caring for a person with bipolar disorder can be time consuming and emotionally challenging. This can lead to financial, physical, and emotional hardships for family or other regular caregivers.28,35,36
Comorbidities
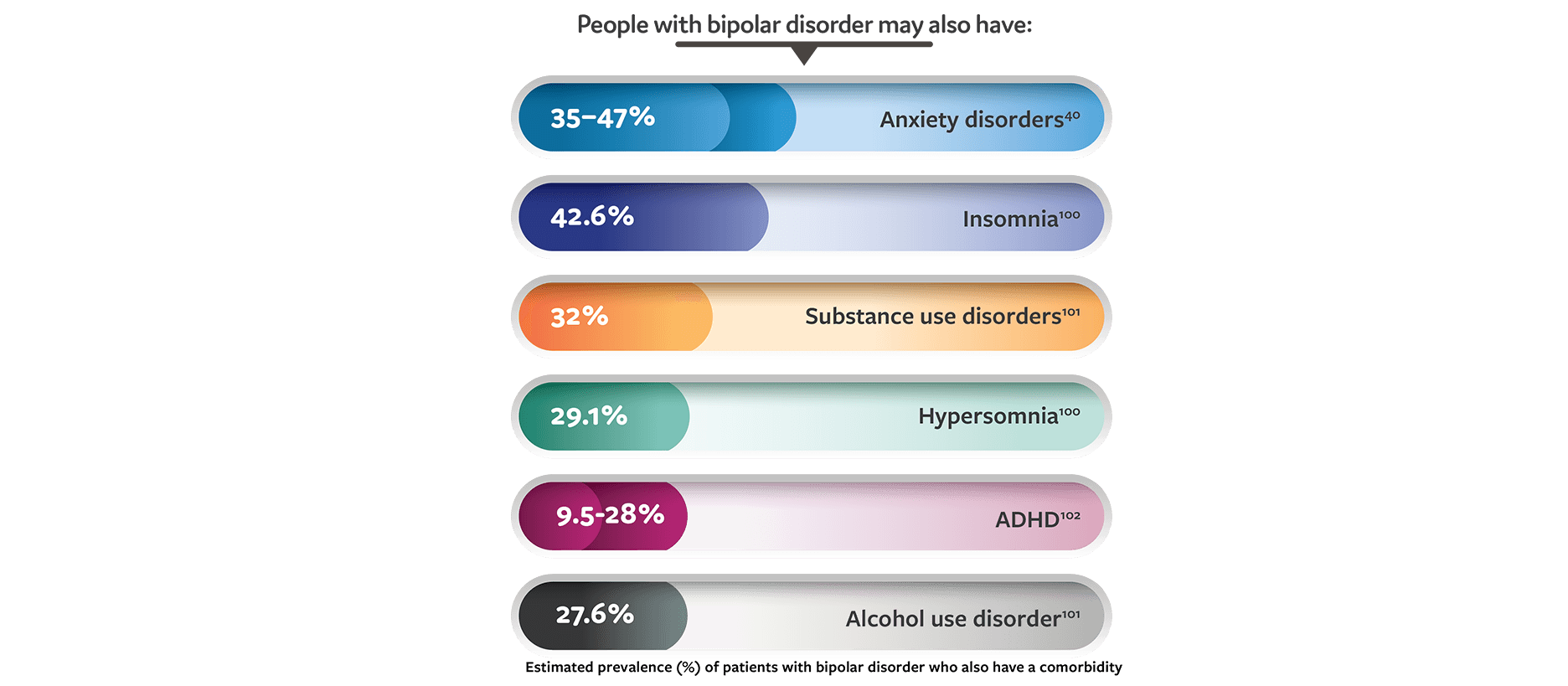
Bipolar disorder is associated with many comorbidities, including hypertension, diabetes, obesity, asthma, migraine, and other psychiatric conditions, including substance use disorders, anxiety disorders, and personality disorders.37 Comorbid psychiatric disorders are associated with poor response to treatment and an increase in symptom severity.22,38-41
Substance use disorders, in particular, are strongly associated with bipolar disorder and can increase cognitive defects.42 They can also complicate treatment by increasing the severity of symptoms and decreasing access to care and treatment adherence.39
Rarely, some medical conditions can cause bipolar disorder, and bipolar disorder symptoms can worsen the original condition and impair treatment.21 While bipolar disorder symptoms may resolve with adequate management of the underlying disease (eg, Cushing’s disease)43,44, people with more permanent conditions (eg, brain injuries) may find it more difficult to manage the symptoms of bipolar disorder.21,45 Other medical conditions that have been found to cause symptoms of bipolar disorder include stroke46, primary psychogenic polydipsia with associated hyponatremia 47, human immunodeficiency virus48, and syphilis.49
Suicide risk
People with bipolar disorder, especially those with predominant depressive episodes, are at a greater risk for suicide.50,51 A 2015 Centers for Disease Control survey of 27 states found that 15.2% of people who completed suicide had a diagnosis of bipolar disorder.52 A large epidemiologic study found the lifetime prevalence of suicide attempts is 20.9% for people with bipolar I disorder and 15.9% for bipolar II disorder53, and another study found that about 7% will have suicidal ideation at least once in their lifetime.54
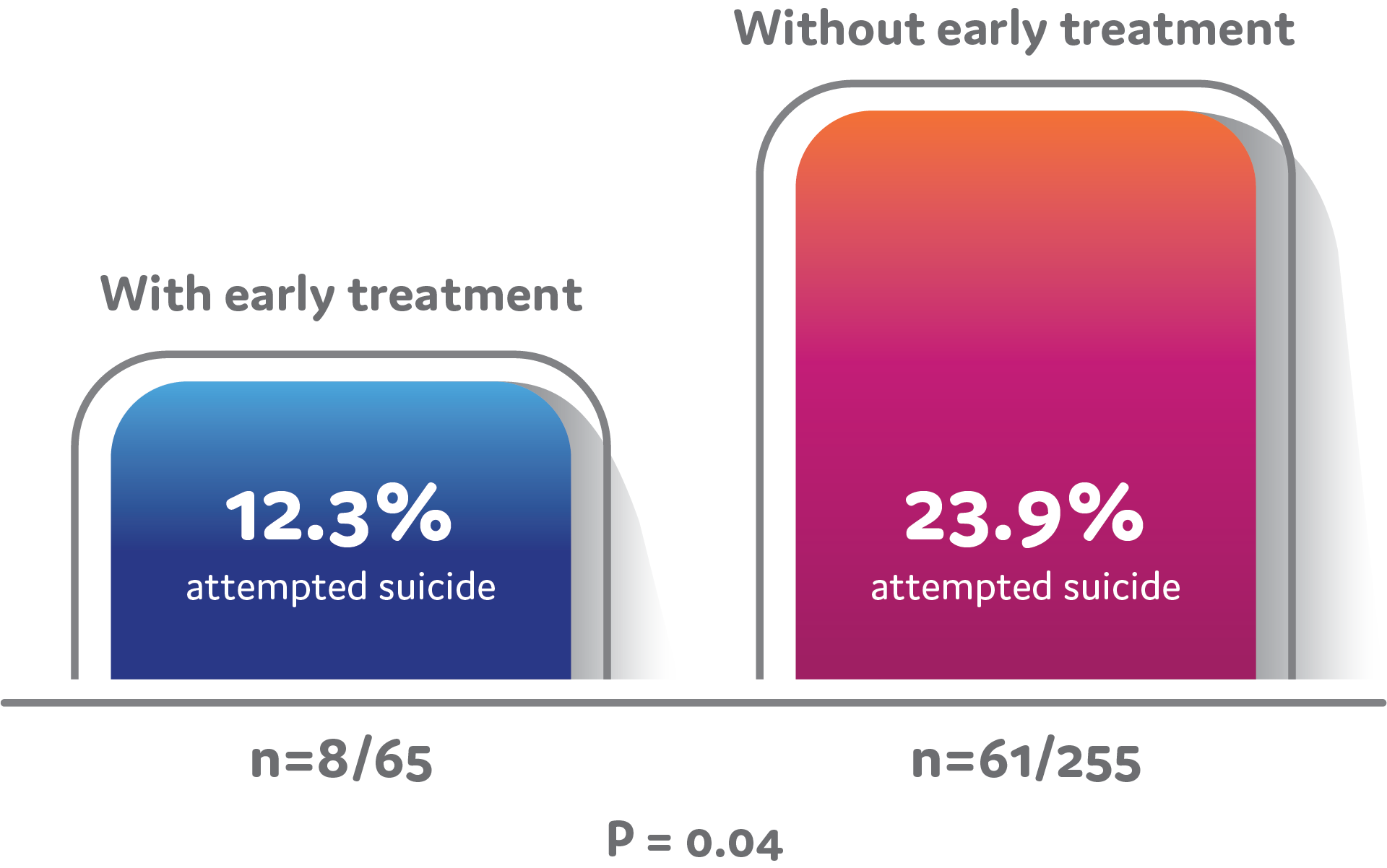
People with bipolar disorder may wait as long as 10 years to receive a correct diagnosis, and delays in receiving adequate treatment can lead to an increased number of suicide attempts and completions (Figure).55 Episodes with depressive features are more strongly associated with an increased number of suicide attempts in people with bipolar disorder.51 People who experience episodes with mixed features have a higher risk of attempting and completing suicide.51,53 It is uncommon for suicide attempts to occur during episodes of mania that do not have any mixed features.51 Because people with bipolar disorder have such an increased risk of suicide, frequently screening patients for potential symptoms is important.22,50 See ‘Diagnosis’ below for more information on screening and assessment.
One study found that the longer a bipolar disorder went untreated, the greater the risk for suicide attempts. People with bipolar disorder who received adequate treatment in 2 years or less from the onset of symptoms had significantly fewer suicide attempts that those who waited longer than 2 years for adequate treatment.56
Diagnosis
Psychiatric comorbidities
Bipolar disorder can also be comorbid with other mental and medical conditions many of which can have similar symptoms.80 It is important that patients receive accurate diagnoses so that they can receive an appropriate treatment option.
While it can be difficult and take time to diagnose a bipolar disorder, your patients will benefit from your persistence, care, and consideration.
Non-Pharmacological Management for Bipolar Disorder
Which lifestyle modifications help with bipolar disorder?
There is no cure for bipolar disorder, but it is treatable.22 Recovery is not an endpoint, but a continuous process that focuses on resilience and staying in control.105 While return to premorbid functioning is not attainable for many patients, investment in actions that boost health and energy, continuing to take medications as prescribed, finding meaning in life, and making life changes can help them lead full lives.22,105,122 Discussing these changes with your patients can help them make the right choices for their needs.
|
|
|
|
|
|
Non-Pharmacological Management for Bipolar Disorder
How can patients plan?
Patients integrate their bipolar disorder diagnosis into their lives and identities in different ways.58 Some share their diagnosis with friends and family to build support networks, while others worry about stigma and prefer to manage their moods privately.130 Regardless of approach, proper planning can help mitigate the more difficult aspects of the illness, such as when a depressive episode leads to suicidal ideation or mania leads to spending sprees.111
Prevention and management tactics can help patients feel better equipped to cope with bipolar disorder. Identifying and controlling stressors, symptoms, and crisis situations can also help patients with bipolar disorder management.111 You can help your patients plan:
|
|
|
|



