MDE Diagnostic Criteria
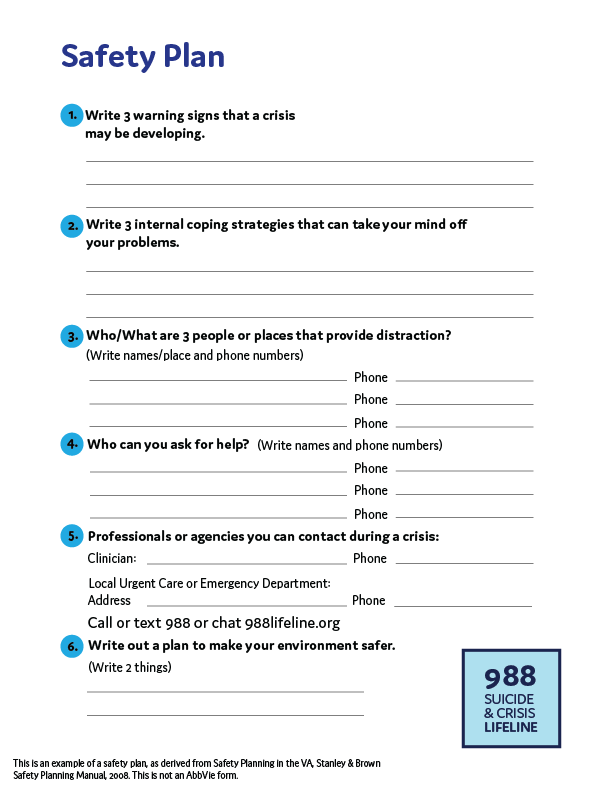
Safety Plan
Key Points
Major Depressive Episode (MDE)
A. Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous function; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
- Depressed mood most of the day, nearly every day, as indicated by either subjective report or observation made by others
- Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day
- Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day
- Insomnia or hypersomnia nearly every day
- Psychomotor agitation or retardation nearly every day
- Fatigue or loss of energy nearly every day
- Feelings of worthlessness or excessive or inappropriate guilt nearly every day
- Diminished ability to think or concentrate, or indecisiveness, nearly every day
- Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide
B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of function
C. The episode is not attributable to the physiological effects of a substance or another medical condition
Diagnostic and Statistical Manual of Mental Disorders. 5th ed.American Psychiatric Association; 2013.
Key Points
- It is important to thoroughly review each of these 9 symptoms with your patients when assessing them for MDD.
- Clinical rating scales can help identify which patients require more in-depth screening for depression.
Watch the video:
APA Guidelines
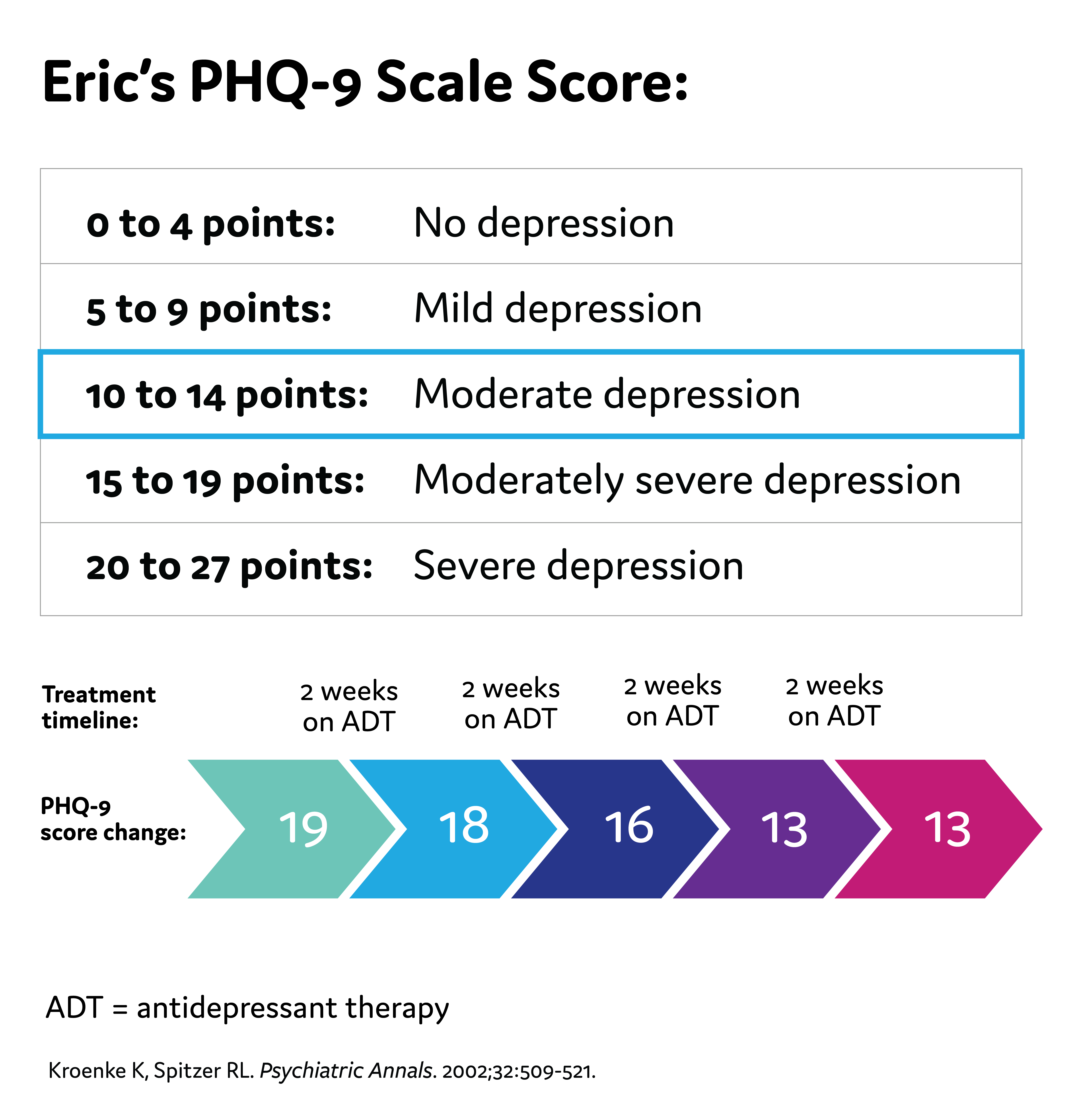
Eric's PHQ-9 Score
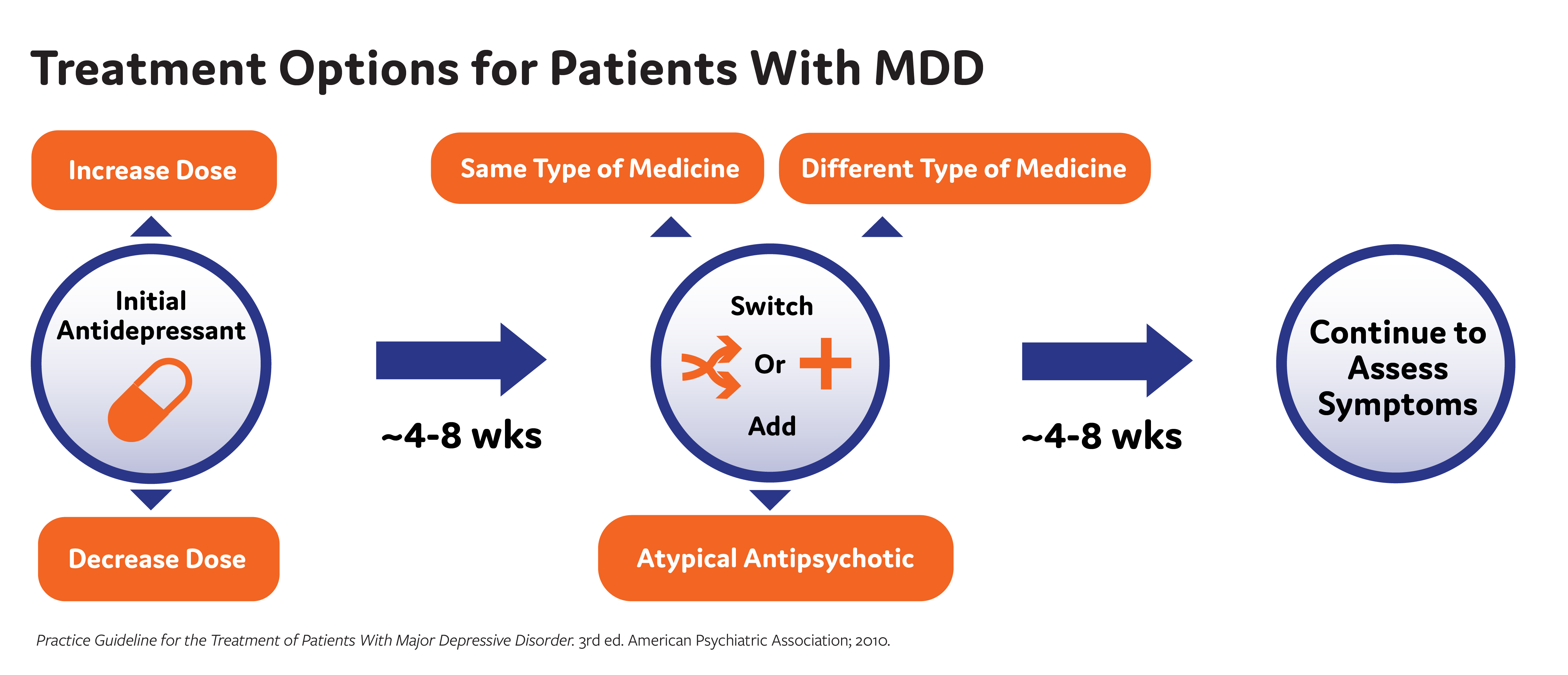
Treatment Options
American Psychiatric Association (APA) Guidelines for Treatment of MDD
1-2 weeks: Improvement from pharmacologic therapy can be seen as early as 1-2 weeks after starting treatment
2-4 weeks: Some patients may achieve improvement in 2-4 weeks
4-6 weeks: Short-term efficacy trials show antidepressant therapy appears to require 4-6 weeks to achieve maximum therapeutic effects
4-8 weeks: The APA recommends 4-8 weeks of adequate* treatment is needed before concluding that a patient is partially responsive or unresponsive to treatment *Adequate dose and duration Practice Guideline for the Treatment of Patients With Major Depressive Disorder. 3rd ed. American Psychiatric Association; 2010.
*Adequate dose and duration
Practice Guideline for the Treatment of Patients with Major Depressive Disorder. 3rd ed. American Psychiatric Association; 2010.
Watch the video:
Treatment Challenges
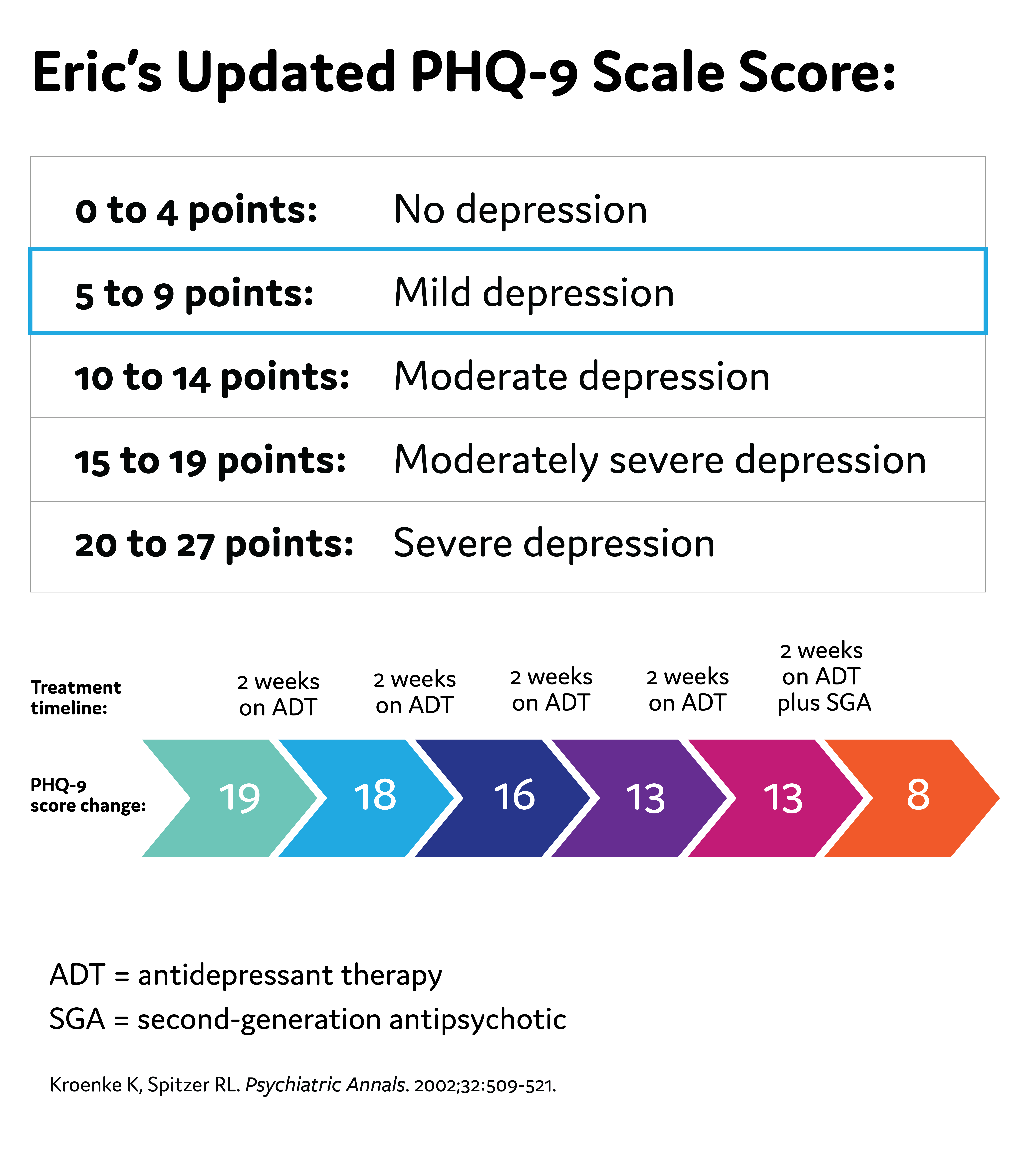
Eric's Updated PHQ-9 Score
Possible Challenges to Antidepressant Therapy
- Suboptimal efficacy due to the wrong dose, inadequate length of time on the medication, or the person's individual biology not being responsive to the medication
- Unpleasant side effects of antidepressants can occur, such as weight gain, insomnia, and sexual dysfunction
- Nonadherence to the antidepressant
- As a reminder, the American Psychiatric Association (APA) recommends 4-8 weeks of adequate* treatment is needed before concluding that a patient is partially responsive or unresponsive to treatment
*Adequate dose and duration
Practice Guideline for the Treatment of Patients With Major Depressive Disorder. 3rd ed. American Psychiatric Association; 2010.
Watch the video:

Tina Matthews-Hayes is a paid consultant for Abbvie Medical Affairs and was compensated for her time.



